This week, mesothelioma clinicians and researchers have come together in Lille, France, for the International Mesothelioma Interest Group‘s biannual meeting known as iMig to discuss mesothelioma treatment updates.
This is a unique meeting where all disciplines come together in one place to discuss all advances, regardless of specialty, in a comprehensive manner. This cross-education of clinicians and scientists is incredibly valuable to future research and patient care.
The first day’s sessions included discussions about mesothelioma treatment updates in epidemiology, imaging, pathology, surgery standardization, and an overview of reported advances from other meetings.
Although so much of the meeting was incredibly technical as it dealt with molecular biology, biomarkers, tumor genetics, etc. during this conference the convergence of advances in biology of mesothelioma and clinical practice was more evident than ever before.
What this means for patients is that as our collective knowledge of mesothelioma and its behavior deepens, clinical researchers take note as they design future clinical trial, and interpret data acquired through previous clinical trials.

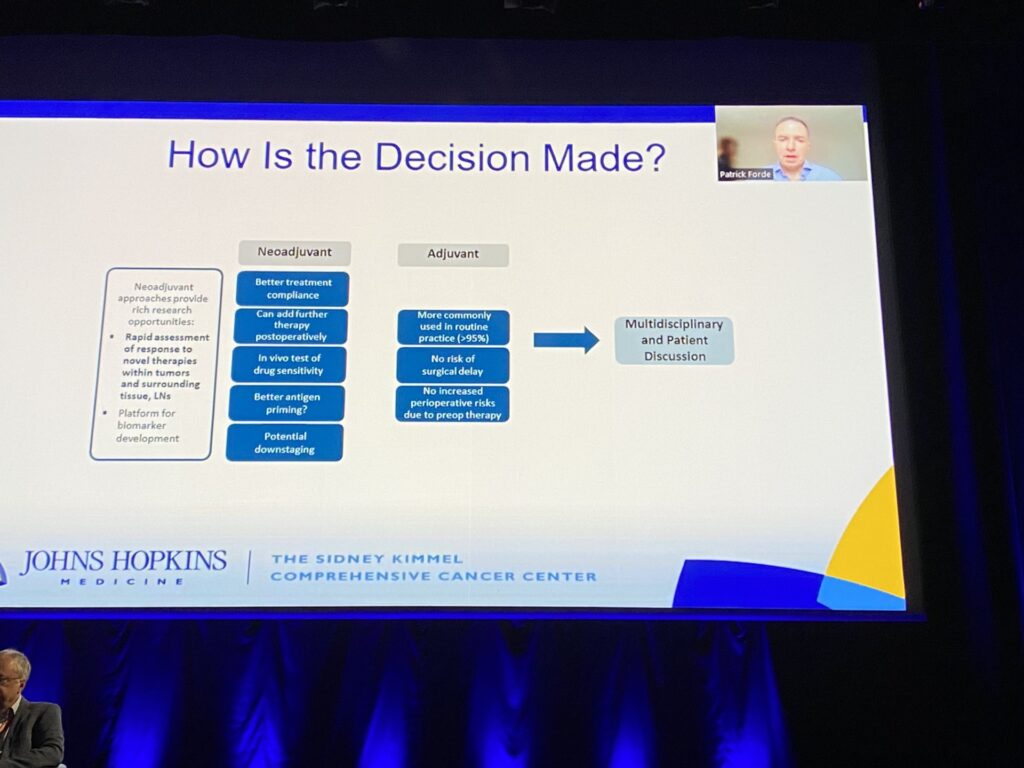
The second day of the conference began with a session addressing questions of vital importance to mesothelioma patients called “Surgery, radiotherapy, neoadjuvant and adjuvant therapies, what is the best combination for multimodal treatment?” The good news is that much work is being done to determine if there is a preferred order to the administration of therapies before and/or after surgery. The bad news is that the answer is not so simple. The work done by Dr. Marc DePerrot with the SMART, SMARTER, and SMARTEST trials, suggests that radiotherapy before surgery is an interesting concept that leads to better outcomes than surgery without radiotherapy. Similarly, Dr. Forde argues that systemic therapy before surgery can be beneficial. One reason is that it allows two options for treatment, one before and the other after surgery. But also it may serve the purpose of “priming” the antigens for subsequent treatment, which would theoretically make it more effective. Finally, treatment before surgery could help downgrade the stage of the cancer making the surgery more effective. One potential downside to treatment before surgery to keep in mind is that it could delay the surgery itself, which is not ideal.
The next session featured the Mesothelioma Applied Research Foundation’s executive director, Julie Powers, as she spoke about the work of the Foundation and how the Foundation meets the needs of mesothelioma patients it serves (including their families).
Presenters also discussed targeted therapies, t cell therapies, peritoneal mesothelioma, patient care and quality of life.
Check this page tomorrow for updates from the last day of the meeting.